What This Medicine Is
REVLIMID is a medicine that helps the immune system and may help stop cancer growth.
Chemical Name
3-(4-amino-1-oxo 1,3-dihydro-2H-isoindol-2-yl) piperidine-2,6-dione
Formula and Weight
The chemical formula is C13H13N3O3.
The molecular weight is 259.3 grams per mole.
What It Looks Like
Lenalidomide is a pale yellow powder. It dissolves in some liquids better than others. It can exist in two different forms (called S and R) that are mixed together.
Available Strengths
REVLIMID comes in capsules of 2.5 mg, 5 mg, 10 mg, 15 mg, 20 mg, and 25 mg.
What’s Inside the Capsule
Each capsule contains lenalidomide (the active medicine) plus these inactive ingredients:
– Lactose anhydrous
– Microcrystalline cellulose
– Croscarmellose sodium
– Magnesium stearate
Capsule Shell
The capsule shell contains gelatin, titanium dioxide, and black ink.
Some strengths also have color additives:
– 5 mg and 25 mg: plain
– 2.5 mg, 10 mg, and 20 mg: blue and yellow color
– 15 mg: blue color
REVLIMID, a thalidomide analogue, is an immunomodulatory agent with antiangiogenic and antineoplastic properties. The chemical name is 3-(4-amino-1-oxo 1,3-dihydro-2H-isoindol-2-yl) piperidine-2,6-dione and it has the following chemical structure:
3-(4-amino-1-oxo 1,3-dihydro-2H-isoindol-2-yl) piperidine-2,6-dione
The empirical formula for lenalidomide is C13H13N3O3, and the gram molecular weight is 259.3.
Lenalidomide is an off-white to pale-yellow solid powder. It is soluble in organic solvent/water mixtures, and buffered aqueous solvents. Lenalidomide is more soluble in organic solvents and low pH solutions. Solubility was significantly lower in less acidic buffers, ranging from about 0.4 to 0.5 mg/ml. Lenalidomide has an asymmetric carbon atom and can exist as the optically active forms S(-) and R(+), and is produced as a racemic mixture with a net optical rotation of zero.
REVLIMID is available in 2.5 mg, 5 mg, 10 mg, 15 mg, 20 mg and 25 mg capsules for oral administration. Each capsule contains lenalidomide as the active ingredient and the following inactive ingredients: lactose anhydrous, microcrystalline cellulose, croscarmellose sodium, and magnesium stearate. The 5 mg and 25 mg capsule shell contains gelatin, titanium dioxide and black ink. The 2.5 mg and 10 mg capsule shell contains gelatin, FD&C blue #2, yellow iron oxide, titanium dioxide and black ink. The 15 mg capsule shell contains gelatin, FD&C blue #2, titanium dioxide and black ink. The 20 mg capsule shell contains gelatin, FD&C blue #2, yellow iron oxide, titanium dioxide and black ink.
Multiple Myeloma Study
A large study tested 3 treatments in 1,623 patients with newly diagnosed multiple myeloma who could not have stem cell transplant:
– Arm Rd Continuous: Revlimid + dexamethasone given until disease got worse
– Arm Rd18: Same medicines for up to 18 cycles (about 72 weeks)
– Arm MPT: Melphalan + prednisone + thalidomide for up to 12 cycles (72 weeks)
Patients took Revlimid 25 mg once daily for 21 days of each 28-day cycle. They also took dexamethasone 40 mg on certain days. Patients over 75 years started with a lower dexamethasone dose of 20 mg. All patients got medicine to prevent blood clots.
Most patients (59%) had early-stage disease. Median age was 73 years. About 35% were over 75. Nine percent had serious kidney problems.
The main goal was to measure progression-free survival (PFS) – time until disease got worse. Results showed Rd Continuous worked better than MPT. Patients on Rd Continuous lived longer without disease getting worse.
—
Mantle Cell Lymphoma Study
A study tested Revlimid alone in patients with mantle cell lymphoma that did not respond to previous treatment. Patients with normal kidneys took Revlimid 25 mg once daily for 21 days of each 28-day cycle.
—
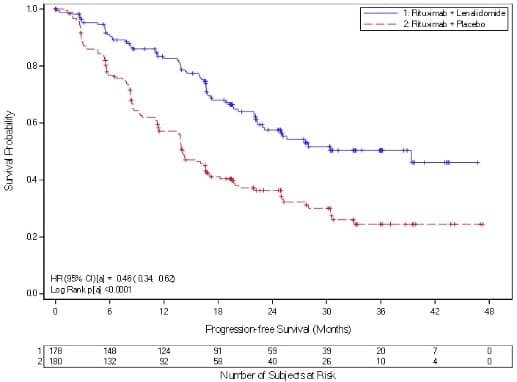
AUGMENT Study – Follicular Lymphoma
In this study, 178 patients got Revlimid + rituximab. Another 180 patients got rituximab + placebo.
Results showed:
– 80% of patients responded to Revlimid + rituximab
– 55% responded to rituximab + placebo
– Median PFS: 39.4 months with Revlimid + rituximab vs 14.1 months with placebo
—
AUGMENT Study – Marginal Zone Lymphoma
In patients with marginal zone lymphoma:
– 65% responded to Revlimid + rituximab
– 44% responded to rituximab + placebo
| CR = complete response; d = low-dose dexamethasone; HR = hazard ratio; IRAC = Independent Response Adjudication Committee; M = melphalan; NE = not estimable; OS = overall survival; P = prednisone; PFS = progression-free survival; PR = partial response; R = REVLIMID; Rd Continuous = Rd given until documentation of progressive disease; Rd18 = Rd given for ≤ 18 cycles; T = thalidomide; VGPR = very good partial response; vs = versus. a The median is based on the Kaplan-Meier estimate. b The 95% Confidence Interval (CI) about the median. c Based on Cox proportional hazards model comparing the hazard functions associated with the indicated treatment arms. d The p-value is based on the unstratified log-rank test of Kaplan-Meier curve differences between the indicated treatment arms. e Best assessment of response during the treatment phase of the study. f Including patients with no response assessment data or whose only assessment was “response not evaluable.” g Data cutoff date = 24 May 2013. h Data cutoff date = 3 March 2014. |
|||
|
Rd Continuous (N = 535) |
Rd18 (N = 541) |
MPT (N = 547) |
|
|
PFS – IRAC (months)g |
|||
|
Number of PFS events |
278 (52) |
348 (64.3) |
334 (61.1) |
|
Mediana PFS time, months (95% CI)b |
25.5 (20.7, 29.4) |
20.7 (19.4, 22) |
21.2 (19.3, 23.2) |
|
HR [95% CI]c; p-valued |
|||
|
Rd Continuous vs MPT |
0.72 (0.61, 0.85); |
||
|
Rd Continuous vs Rd18 |
0.70 (0.60, 0.82) |
||
|
Rd18 vs MPT |
1.03 (0.89, 1.20) |
||
|
Overall Survival (months)h |
|||
|
Number of Death events |
208 (38.9) |
228 (42.1) |
261 (47.7) |
|
Mediana OS time, months (95% CI)b |
58.9 (56, NE)f |
56.7 (50.1, NE) |
48.5 (44.2, 52 ) |
|
HR [95% CI]c |
|||
|
Rd Continuous vs MPT |
0.75 (0.62, 0.90) |
||
|
Rd Continuous vs Rd18 |
0.91 (0.75, 1.09) |
||
|
Rd18 vs MPT |
0.83 (0.69, 0.99) |
||
|
Response Ratee – IRAC, n (%)g |
|||
|
CR |
81 (15.1) |
77 (14.2) |
51 (9.3) |
|
VGPR |
152 (28.4) |
154 (28.5) |
103 (18.8) |
|
PR |
169 (31.6) |
166 (30.7) |
187 (34.2) |
|
Overall response: CR, VGPR, or PR |
402 (75.1) |
397 (73.4) |
341 (62.3) |
| Data cutoff date = 1 March 2015. | ||||
|
Maintenance Study 1 |
Maintenance Study 2 |
|||
|
REVLIMID N = 231 |
Placebo N = 229 |
REVLIMID N = 307 |
Placebo N = 307 |
|
|
Age (years) |
||||
|
Median |
58 |
58 |
57.5 |
58.1 |
|
(Min, max) |
(29, 71) |
(39, 71) |
(22.7, 68.3) |
(32.3, 67) |
|
Sex, n (%) |
||||
|
Male |
121 (52) |
129 (56) |
169 (55) |
181 (59) |
|
Female |
110 (48) |
100 (44) |
138 (45) |
126 (41) |
|
ISS Stage at Diagnosis, n (%) |
||||
|
Stage I or II |
120 (52) |
131 (57) |
232 (76) |
250 (81) |
|
Stage I |
62 (27) |
85 (37) |
128 (42) |
143 (47) |
|
Stage II |
58 (25) |
46 (20) |
104 (34) |
107 (35) |
|
Stage III |
39 (17) |
35 (15) |
66 (21) |
46 (15) |
|
Missing |
72 (31) |
63 (28) |
9 (3) |
11 (4) |
|
CrCl at Post-auto-HSCT, n (%) |
||||
|
< 50 mL/min |
23 (10) |
16 (7) |
10 (3) |
9 (3) |
|
≥ 50 mL/min |
201 (87) |
204 (89) |
178 (58) |
200 (65) |
|
Missing |
7 (3) |
9 (4) |
119 (39) |
98 (32) |
| Date of Unblinding in Maintenance Study 1 and 2 = 17 December 2009 and 7 July 2010, respectively. Auto-HSCT = autologous hematopoietic stem cell transplantation; CI = confidence interval; ITT = intent to treat; NE = not estimable; PFS = progression-free survival. PFS at time of unblinding for Maintenance Study 2 was based on assessment by an Independent Review Committee. All other PFS analyses were based on assessment by investigator. Note: The median is based on Kaplan-Meier estimate, with 95% CIs about the median overall PFS time. Hazard ratio is based on a proportional hazards model stratified by stratification factors comparing the hazard functions associated with treatment arms (REVLIMID:placebo). |
||||
|
Maintenance Study 1 |
Maintenance Study 2 |
|||
|
REVLIMID N = 231 |
Placebo N = 229 |
REVLIMID N = 307 |
Placebo N = 307 |
|
|
PFS at Unblinding |
||||
|
PFS Events n (%) |
46 (20) |
98 (43) |
103 (34) |
160 (52) |
|
Median in months [95% CI] |
33.9 |
19 |
41.2 |
23.0 |
|
Hazard Ratio |
0.38 |
0.50 |
||
|
Log-rank Test p-value |
<0.001 |
<0.001 |
||
|
PFS at Updated Analysis 1 March 2015 (Studies 1 and 2) |
||||
|
PFS Events n (%) |
97 (42) |
116 (51) |
191 (62) |
248 (81) |
|
Median in months [95% CI] |
68.6 |
22.5 |
46.3 |
23.8 |
|
Hazard Ratio |
0.38 |
0.53 |
||
|
OS at Updated Analysis 1 Feb 2016 (Studies 1 and 2) |
||||
|
OS Events n (%) |
82 (35) |
114 (50) |
143 (47) |
160 (52) |
|
Median in months [95% CI] |
111 |
84.2 |
105.9 |
88.1 |
|
Hazard Ratio |
0.59 |
0.90 |
||
|
Study 1 |
Study 2 |
|||
|
REVLIMID/Dex N=177 |
Placebo/Dex N=176 |
REVLIMID/Dex N=176 |
Placebo/Dex N=175 |
|
|
Patient Characteristics |
||||
|
Age (years) |
||||
|
Median |
64 |
62 |
63 |
64 |
|
Min, Max |
36, 86 |
37, 85 |
33, 84 |
40, 82 |
|
Sex |
||||
|
Male |
106 (60%) |
104 (59%) |
104 (59%) |
103 (59%) |
|
Female |
71 (40%) |
72 (41%) |
72 (41%) |
72 (41%) |
|
Race/Ethnicity |
||||
|
White |
141(80%) |
148 (84%) |
172 (98%) |
175 (100%) |
|
Other |
36 (20%) |
28 (16%) |
4 (2%) |
0 (0%) |
|
ECOG Performance |
||||
|
Status 0-1 |
157 (89%) |
168 (95%) |
150 (85%) |
144 (82%) |
|
Disease Characteristics |
||||
|
Multiple Myeloma Stage (Durie-Salmon) |
||||
|
I |
3% |
3% |
6% |
5% |
|
II |
32% |
31% |
28% |
33% |
|
III |
64% |
66% |
65% |
63% |
|
β2-microglobulin (mg/L) |
||||
|
≤ 2.5 mg/L |
52 (29%) |
51 (29%) |
51 (29%) |
48 (27%) |
|
> 2.5 mg/L |
125 (71%) |
125 (71%) |
125 (71%) |
127 (73%) |
|
Number of Prior Therapies |
||||
|
1 |
38% |
38% |
32% |
33% |
|
≥ 2 |
62% |
62% |
68% |
67% |
|
Types of Prior Therapies |
||||
|
Stem Cell Transplantation |
62% |
61% |
55% |
54% |
|
Thalidomide |
42% |
46% |
30% |
38% |
|
Dexamethasone |
81% |
71% |
66% |
69% |
|
Bortezomib |
11% |
11% |
5% |
4% |
|
Melphalan |
33% |
31% |
56% |
52% |
|
Doxorubicin |
55% |
51% |
56% |
57% |
|
Study 1 |
Study 2 |
|||
|
REVLIMID/Dex N=177 |
Placebo/Dex N=176 |
REVLIMID/Dex N=176 |
Placebo/Dex N=175 |
|
|
TTP |
||||
|
Events n (%) |
73 (41) |
120 (68) |
68 (39) |
130 (74) |
|
Median TTP in months [95% CI] |
13.9 |
4.7 |
12.1 |
4.7 |
|
Hazard Ratio |
0.285 |
0.324 |
||
|
Log-rank Test p-value 3 |
<0.001 |
<0.001 |
||
|
Response |
||||
|
Complete Response (CR) n (%) |
23 (13) |
1 (1) |
27 (15) |
7 (4) |
|
Partial Response (RR/PR) n (%) |
84 (48) |
33 (19) |
77 (44) |
34 (19) |
|
Overall Response n (%) |
107 (61) |
34 (19) |
104 (59) |
41 (23) |
|
p-value |
<0.001 |
<0.001 |
||
|
Odds Ratio [95% CI] |
6.38 |
4.72 |
||
| a IPSS Risk Category: Low (combined score = 0), Intermediate-1 (combined score = 0.5 to 1), Intermediate-2 (combined score = 1.5 to 2.0), High (combined score ≥ 2.5); Combined score = (Marrow blast score + Karyotype score + Cytopenia score). b French-American-British (FAB) classification of MDS. |
||
|
Overall (N=148) |
||
|
Age (years) |
||
|
Median |
71 |
|
|
Min, Max |
37, 95 |
|
|
Gender |
n |
(%) |
|
Male |
51 |
(34.5) |
|
Female |
97 |
(65.5) |
|
Race |
n |
(%) |
|
White |
143 |
(96.6) |
|
Other |
5 |
( 3.4) |
|
Duration of MDS (years) |
||
|
Median |
2.5 |
|
|
Min, Max |
0.1, 20.7 |
|
|
Del 5 (q31-33) Cytogenetic Abnormality |
n |
(%) |
|
Yes |
148 |
(100) |
|
Other cytogenetic abnormalities |
37 |
(25.2) |
|
IPSS Score a |
n |
(%) |
|
Low (0) |
55 |
(37.2) |
|
Intermediate-1 (0.5-1.0) |
65 |
(43.9) |
|
Intermediate-2 (1.5-2.0) |
6 |
( 4.1) |
|
High (≥2.5) |
2 |
( 1.4) |
|
Missing |
20 |
(13.5) |
|
FAB Classification b from central review |
n |
(%) |
|
RA |
77 |
(52) |
|
RARS |
16 |
(10.8) |
|
RAEB |
30 |
(20.3) |
|
CMML |
3 |
( 2) |
| a ECOG = Eastern Cooperative Oncology Group. b MIPI = MCL International Prognostic Index. c High tumor burden is defined as at least one lesion that is ≥5 cm in diameter or 3 lesions that are ≥3 cm in diameter. d Bulky disease is defined as at least one lesion that is ≥7cm in the longest diameter. |
|
|
Baseline Disease Characteristics and Prior Anti -Lymphoma Treatment |
Total Patients (N=134) |
|
ECOG Performance Statusa n (%) |
|
|
0 |
43 (32) |
|
1 |
73 (54) |
|
2 |
17 (13) |
|
3 |
1 (<1) |
|
Advanced MCL Stage, n (%) |
|
|
III |
27 (20) |
|
IV |
97 (72) |
|
High or Intermediate MIPI Score b, n (%) |
90 (67) |
|
High Tumor Burdenc, n (%) |
77 (57) |
|
Bulky Diseased, n (%) |
44 (33) |
|
Extranodal Disease, n (%) |
101 (75) |
|
Number of Prior Systemic Anti-Lymphoma Therapies, n (%) |
|
|
Median (range) |
4 (2, 10) |
|
1 |
0 (0) |
|
2 |
29 (22) |
|
3 |
34 (25) |
|
≥ 4 |
71 (53) |
|
Number of Subjects Who Received Prior Regimen Containing, n (%): |
|
|
Anthracycline/mitoxantrone |
133 (99) |
|
Cyclophosphamide |
133 (99) |
|
Rituximab |
134 (100) |
|
Bortezomib |
134 (100) |
|
Refractory to Prior Bortezomib, n (%) |
81 (60) |
|
Refractory to Last Prior Therapy, n (%) |
74 (55) |
|
Prior Autologous Bone Marrow or Stem Cell Transplant, n (%) |
39 (29) |
|
Response Analyses (N = 133) |
N (%) |
95% CI |
|
|
Overall Response Rate (IWRC) (CR + CRu +PR) |
34 (26) |
(18.4, 33.9) |
|
|
Complete Response (CR + CRu) |
9 (7) |
(3.1, 12.5) |
|
|
CR |
1 (1) |
||
|
CRu |
8 (6) |
||
|
Partial Response (PR) |
25 (19) |
||
|
Duration of Response (months) |
Median |
95% CI |
|
|
Duration of Overall Response (CR + CRu + PR) |
(N = 34) |
16.6 |
(7.7, 26.7) |
| Data Cutoff: 22 June 2018 (AUGMENT) and 1 May 2017 (MAGNIFY). a Defined by GELF criteria. b Patient had either 0 (n=2) or 1 prior systemic therapy. ECOG = Eastern Cooperative Oncology Group; FLIPI = follicular lymphoma international prognostic index |
|||
|
Parameter |
AUGMENT Trial |
MAGNIFY Trial |
|
|
REVLIMID + Rituximab (N=178) |
Rituximab + Placebo (Control Arm) (N=180) |
REVLIMID + Rituximab (N=222) |
|
|
Age (years) |
|||
|
Median (Max, Min) |
64 (26, 86) |
62 (35, 88) |
65 (35, 91) |
|
Age distribution, n (%) |
|||
|
<65 years |
96 (54) |
107 (59) |
103 (46) |
|
≥65 years |
82 (46) |
73 (41) |
119 (54) |
|
Sex, n (%) |
|||
|
Male |
75 (42) |
97 (54) |
122 (55) |
|
Female |
103 (58) |
83 (46) |
100 (45) |
|
Race |
|||
|
White |
118 (66) |
115 (64) |
206 (93) |
|
Other races |
54 (30) |
64 (36) |
14 (6) |
|
Not collected or reported |
6 (3) |
1 (0.6) |
2 (1) |
|
Body Surface Area (BSA, m2) |
|||
|
Median (Max, Min) |
1.8 (1.4, 3.1) |
1.8 (1.3, 2.7) |
2 (1.3, 2.6) |
|
Disease Type FL or MZL |
|||
|
Follicular lymphoma |
147 (83) |
148 (82) |
177 (80) |
|
Marginal zone lymphoma |
31 (17) |
32 (18) |
45 (20) |
|
MZL subtype at diagnosis (investigator), n (%) |
|||
|
MALT |
14 (45) |
16 (50) |
10 (22) |
|
Nodal |
8 (26) |
10 (31) |
25 (56) |
|
Splenic |
9 (29) |
6 (19) |
10 (22) |
|
FL stage at diagnosis (investigator), n (%) |
|||
|
FL Grade 1-2 |
125 (85) |
123 (83) |
149 (84) |
|
FL Grade 3a |
22 (15) |
25 (17) |
28 (16) |
|
FLIPI score at baseline (calculated), n (%) |
Not Collected |
||
|
Low risk (0,1) |
52 (29) |
67 (37) |
|
|
Intermediate risk (2) |
55 (31) |
58 (32) |
|
|
High risk (≥3) |
69 (39) |
54 (30) |
|
|
Missing |
2 (1) |
1 (0.6) |
|
|
ECOG score at baseline, n (%) |
|||
|
0 |
116 (65) |
128 (71) |
102 (46) |
|
1 |
60 (34) |
50 (28) |
113 (51) |
|
2 |
2 (1) |
2 (1) |
7 (3) |
|
High tumor burdena at baseline, n (%) |
|||
|
Yes |
97 (54) |
86 (48) |
148 (67) |
|
No |
81 (46) |
94 (52) |
74 (33) |
|
Number of prior systemic antilymphoma therapies |
|||
|
1 |
102 (57) |
97 (54) |
94 (42)b |
|
>1 |
76 (43) |
83 (46) |
128 (58) |
| a Median estimate is from Kaplan-Meier analysis. b hazard ratio and its CI were estimated from Cox proportional hazard model adjusting for the stratification 3: previous rituximab treatment (yes, no), time since last antilymphoma therapy (≤ 2, > 2 years), and disease histology (FL, MZL). c p-value from log-rank test stratified by 3 factors noted above: previous rituximab treatment (yes, no), time since last antilymphoma therapy (≤ 2, > 2 years), and disease histology (FL, MZL). d Exact confidence interval for binomial distribution. |
||
|
Parameter |
REVLIMID + Rituximab (N=178) |
Rituximab + Placebo (N=180) |
|
PFS |
||
|
Patients with event, n (%) |
68 (38.2) |
115 (63.9) |
|
Death |
6 (8.8) |
2 (1.7) |
|
Progression of disease |
62 (91.2) |
113 (98.3) |
|
PFS, median a [95% CI] (months) |
39.4 [ 22.9, NE] |
14.1 [11.4, 16.7] |
|
HR b [95% CI] |
0.46 [ 0.34, 0.62] |
|
|
p-value c |
<0.0001 |
|
|
Objective response (CR+PR) , n(%) [95% CI] d |
138 (77.5) [70.7, 83.4] |
96 (53.3) [45.8, 60.8] |
14.1 Multiple Myeloma
Randomized, Open-Label Clinical Trial in Patients with Newly Diagnosed MM:
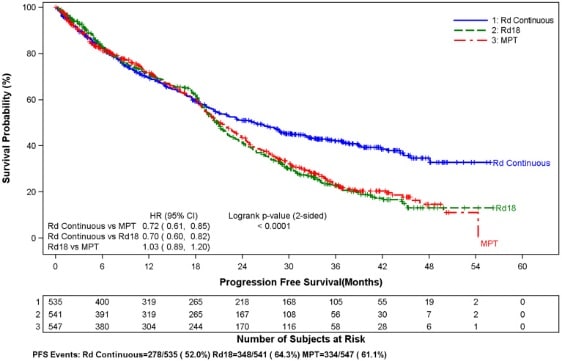
A randomized multicenter, open-label, 3-arm trial of 1,623 patients, was conducted to compare the efficacy and safety of REVLIMID and low-dose dexamethasone (Rd) given for 2 different durations of time to that of melphalan, prednisone and thalidomide (MPT) in newly diagnosed MM patients who were not a candidate for stem cell transplant. In the first arm of the study, Rd was given continuously until progressive disease [Arm Rd Continuous]. In the second arm, Rd was given for up to eighteen 28-day cycles [72 weeks, Arm Rd18]). In the third arm, melphalan, prednisone and thalidomide (MPT) was given for a maximum of twelve 42-day cycles (72 weeks). For the purposes of this study, a patient who was 75 years), stage (ISS Stages I and II versus Stage III), and country.
Patients in the Rd Continuous and Rd18 arms received REVLIMID 25 mg once daily on Days 1 to 21 of 28-day cycles. Dexamethasone was dosed 40 mg once daily on Days 1, 8, 15, and 22 of each 28-day cycle. For patients over > 75 years old, the starting dose of dexamethasone was 20 mg orally once daily on days 1,8,15, and 22 of repeated 28-day cycles. Initial dose and regimens for Rd Continuous and Rd18 were adjusted according to age and renal function. All patients received prophylactic anticoagulation with the most commonly used being aspirin.
The demographics and disease-related baseline characteristics of the patients were balanced among the 3 arms. In general, study subjects had advanced-stage disease. Of the total study population, the median age was 73 in the 3 arms with 35% of total patients > 75 years of age; 59% had ISS Stage I/II; 41% had ISS stage III; 9% had severe renal impairment (creatinine clearance [CLcr] 30 to 50 mL/min; 44% had mild renal impairment (CLcr > 50 to 80 mL/min). For ECOG Performance Status, 29% were Grade 0, 49% Grade 1, 21% Grade 2, 0.4% ≥ Grade 3.
The primary efficacy endpoint, progression-free survival (PFS), was defined as the time from randomization to the first documentation of disease progression as determined by Independent Response Adjudication Committee (IRAC), based on International Myeloma Working Group [IMWG] criteria or death due to any cause, whichever occurred first during the study until the end of the PFS follow-up phase. For the efficacy analysis of all endpoints, the primary comparison was between Rd Continuous and MPT arms. The efficacy results are summarized in the table below. PFS was significantly longer with Rd Continuous than MPT: HR 0.72 (95% CI: 0.61-0.85 p 2.5 mg/L
125 (71%)
125 (71%)
125 (71%)
127 (73%)
Number of Prior Therapies
1
38%
38%
32%
33%
≥ 2
62%
62%
68%
67%
Types of Prior Therapies
Stem Cell Transplantation
62%
61%
55%
54%
Thalidomide
42%
46%
30%
38%
Dexamethasone
81%
71%
66%
69%
Bortezomib
11%
11%
5%
4%
Melphalan
33%
31%
56%
52%
Doxorubicin
55%
51%
56%
57%
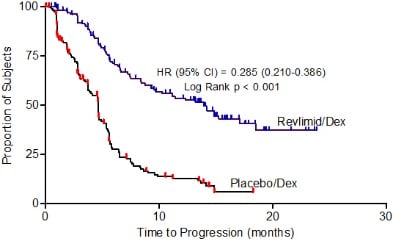
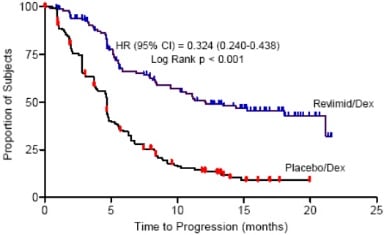
The primary efficacy endpoint in both studies was time to progression (TTP). TTP was defined as the time from randomization to the first occurrence of progressive disease.
Preplanned interim analyses of both studies showed that the combination of REVLIMID/dexamethasone was significantly superior to dexamethasone alone for TTP. The studies were unblinded to allow patients in the placebo/dexamethasone group to receive treatment with the REVLIMID/dexamethasone combination. For both studies, the extended follow-up survival data with crossovers were analyzed. In study 1, the median survival time was 39.4 months (95%CI: 32.9, 47.4) in REVLIMID/dexamethasone group and 31.6 months (95% CI: 24.1, 40.9) in placebo/dexamethasone group, with a hazard ratio of 0.79 (95% CI: 0.61-1.03). In study 2, the median survival time was 37.5 months (95%CI: 29.9, 46.6) in REVLIMID/dexamethasone group and 30.8 months (95%CI: 23.5, 40.3) in placebo/dexamethasone group, with a hazard ratio of 0.86 (95% CI: 0.65-1.14).
| CR = complete response; d = low-dose dexamethasone; HR = hazard ratio; IRAC = Independent Response Adjudication Committee; M = melphalan; NE = not estimable; OS = overall survival; P = prednisone; PFS = progression-free survival; PR = partial response; R = REVLIMID; Rd Continuous = Rd given until documentation of progressive disease; Rd18 = Rd given for ≤ 18 cycles; T = thalidomide; VGPR = very good partial response; vs = versus. a The median is based on the Kaplan-Meier estimate. b The 95% Confidence Interval (CI) about the median. c Based on Cox proportional hazards model comparing the hazard functions associated with the indicated treatment arms. d The p-value is based on the unstratified log-rank test of Kaplan-Meier curve differences between the indicated treatment arms. e Best assessment of response during the treatment phase of the study. f Including patients with no response assessment data or whose only assessment was “response not evaluable.” g Data cutoff date = 24 May 2013. h Data cutoff date = 3 March 2014. |
|||
|
Rd Continuous (N = 535) |
Rd18 (N = 541) |
MPT (N = 547) |
|
|
PFS – IRAC (months)g |
|||
|
Number of PFS events |
278 (52) |
348 (64.3) |
334 (61.1) |
|
Mediana PFS time, months (95% CI)b |
25.5 (20.7, 29.4) |
20.7 (19.4, 22) |
21.2 (19.3, 23.2) |
|
HR [95% CI]c; p-valued |
|||
|
Rd Continuous vs MPT |
0.72 (0.61, 0.85); |
||
|
Rd Continuous vs Rd18 |
0.70 (0.60, 0.82) |
||
|
Rd18 vs MPT |
1.03 (0.89, 1.20) |
||
|
Overall Survival (months)h |
|||
|
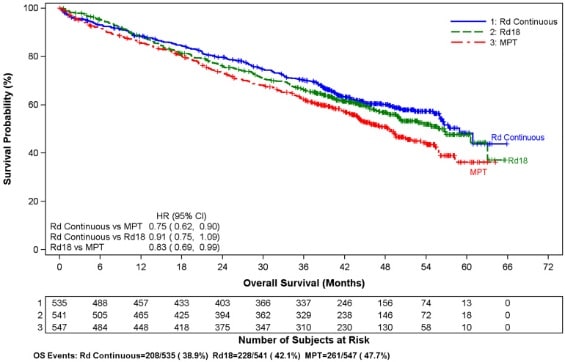
Number of Death events |
208 (38.9) |
228 (42.1) |
261 (47.7) |
|
Mediana OS time, months (95% CI)b |
58.9 (56, NE)f |
56.7 (50.1, NE) |
48.5 (44.2, 52 ) |
|
HR [95% CI]c |
|||
|
Rd Continuous vs MPT |
0.75 (0.62, 0.90) |
||
|
Rd Continuous vs Rd18 |
0.91 (0.75, 1.09) |
||
|
Rd18 vs MPT |
0.83 (0.69, 0.99) |
||
|
Response Ratee – IRAC, n (%)g |
|||
|
CR |
81 (15.1) |
77 (14.2) |
51 (9.3) |
|
VGPR |
152 (28.4) |
154 (28.5) |
103 (18.8) |
|
PR |
169 (31.6) |
166 (30.7) |
187 (34.2) |
|
Overall response: CR, VGPR, or PR |
402 (75.1) |
397 (73.4) |
341 (62.3) |
| Data cutoff date = 1 March 2015. | ||||
|
Maintenance Study 1 |
Maintenance Study 2 |
|||
|
REVLIMID N = 231 |
Placebo N = 229 |
REVLIMID N = 307 |
Placebo N = 307 |
|
|
Age (years) |
||||
|
Median |
58 |
58 |
57.5 |
58.1 |
|
(Min, max) |
(29, 71) |
(39, 71) |
(22.7, 68.3) |
(32.3, 67) |
|
Sex, n (%) |
||||
|
Male |
121 (52) |
129 (56) |
169 (55) |
181 (59) |
|
Female |
110 (48) |
100 (44) |
138 (45) |
126 (41) |
|
ISS Stage at Diagnosis, n (%) |
||||
|
Stage I or II |
120 (52) |
131 (57) |
232 (76) |
250 (81) |
|
Stage I |
62 (27) |
85 (37) |
128 (42) |
143 (47) |
|
Stage II |
58 (25) |
46 (20) |
104 (34) |
107 (35) |
|
Stage III |
39 (17) |
35 (15) |
66 (21) |
46 (15) |
|
Missing |
72 (31) |
63 (28) |
9 (3) |
11 (4) |
|
CrCl at Post-auto-HSCT, n (%) |
||||
|
< 50 mL/min |
23 (10) |
16 (7) |
10 (3) |
9 (3) |
|
≥ 50 mL/min |
201 (87) |
204 (89) |
178 (58) |
200 (65) |
|
Missing |
7 (3) |
9 (4) |
119 (39) |
98 (32) |
| Date of Unblinding in Maintenance Study 1 and 2 = 17 December 2009 and 7 July 2010, respectively. Auto-HSCT = autologous hematopoietic stem cell transplantation; CI = confidence interval; ITT = intent to treat; NE = not estimable; PFS = progression-free survival. PFS at time of unblinding for Maintenance Study 2 was based on assessment by an Independent Review Committee. All other PFS analyses were based on assessment by investigator. Note: The median is based on Kaplan-Meier estimate, with 95% CIs about the median overall PFS time. Hazard ratio is based on a proportional hazards model stratified by stratification factors comparing the hazard functions associated with treatment arms (REVLIMID:placebo). |
||||
|
Maintenance Study 1 |
Maintenance Study 2 |
|||
|
REVLIMID N = 231 |
Placebo N = 229 |
REVLIMID N = 307 |
Placebo N = 307 |
|
|
PFS at Unblinding |
||||
|
PFS Events n (%) |
46 (20) |
98 (43) |
103 (34) |
160 (52) |
|
Median in months [95% CI] |
33.9 |
19 |
41.2 |
23.0 |
|
Hazard Ratio |
0.38 |
0.50 |
||
|
Log-rank Test p-value |
<0.001 |
<0.001 |
||
|
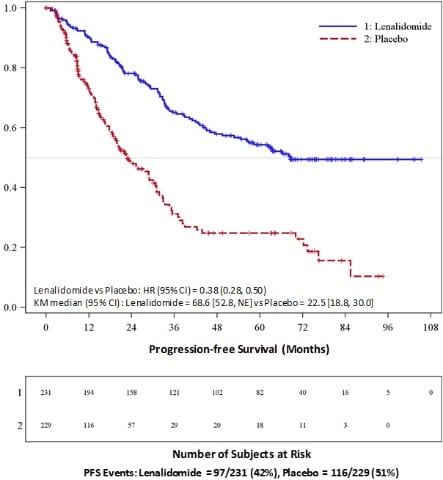
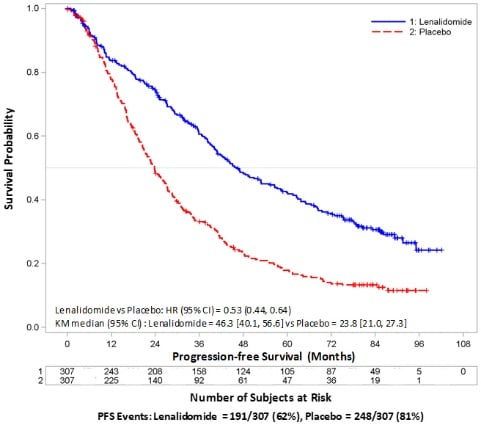
PFS at Updated Analysis 1 March 2015 (Studies 1 and 2) |
||||
|
PFS Events n (%) |
97 (42) |
116 (51) |
191 (62) |
248 (81) |
|
Median in months [95% CI] |
68.6 |
22.5 |
46.3 |
23.8 |
|
Hazard Ratio |
0.38 |
0.53 |
||
|
OS at Updated Analysis 1 Feb 2016 (Studies 1 and 2) |
||||
|
OS Events n (%) |
82 (35) |
114 (50) |
143 (47) |
160 (52) |
|
Median in months [95% CI] |
111 |
84.2 |
105.9 |
88.1 |
|
Hazard Ratio |
0.59 |
0.90 |
||
|
Study 1 |
Study 2 |
|||
|
REVLIMID/Dex N=177 |
Placebo/Dex N=176 |
REVLIMID/Dex N=176 |
Placebo/Dex N=175 |
|
|
Patient Characteristics |
||||
|
Age (years) |
||||
|
Median |
64 |
62 |
63 |
64 |
|
Min, Max |
36, 86 |
37, 85 |
33, 84 |
40, 82 |
|
Sex |
||||
|
Male |
106 (60%) |
104 (59%) |
104 (59%) |
103 (59%) |
|
Female |
71 (40%) |
72 (41%) |
72 (41%) |
72 (41%) |
|
Race/Ethnicity |
||||
|
White |
141(80%) |
148 (84%) |
172 (98%) |
175 (100%) |
|
Other |
36 (20%) |
28 (16%) |
4 (2%) |
0 (0%) |
|
ECOG Performance |
||||
|
Status 0-1 |
157 (89%) |
168 (95%) |
150 (85%) |
144 (82%) |
|
Disease Characteristics |
||||
|
Multiple Myeloma Stage (Durie-Salmon) |
||||
|
I |
3% |
3% |
6% |
5% |
|
II |
32% |
31% |
28% |
33% |
|
III |
64% |
66% |
65% |
63% |
|
β2-microglobulin (mg/L) |
||||
|
≤ 2.5 mg/L |
52 (29%) |
51 (29%) |
51 (29%) |
48 (27%) |
|
> 2.5 mg/L |
125 (71%) |
125 (71%) |
125 (71%) |
127 (73%) |
|
Number of Prior Therapies |
||||
|
1 |
38% |
38% |
32% |
33% |
|
≥ 2 |
62% |
62% |
68% |
67% |
|
Types of Prior Therapies |
||||
|
Stem Cell Transplantation |
62% |
61% |
55% |
54% |
|
Thalidomide |
42% |
46% |
30% |
38% |
|
Dexamethasone |
81% |
71% |
66% |
69% |
|
Bortezomib |
11% |
11% |
5% |
4% |
|
Melphalan |
33% |
31% |
56% |
52% |
|
Doxorubicin |
55% |
51% |
56% |
57% |
|
Study 1 |
Study 2 |
|||
|
REVLIMID/Dex N=177 |
Placebo/Dex N=176 |
REVLIMID/Dex N=176 |
Placebo/Dex N=175 |
|
|
TTP |
||||
|
Events n (%) |
73 (41) |
120 (68) |
68 (39) |
130 (74) |
|
Median TTP in months [95% CI] |
13.9 |
4.7 |
12.1 |
4.7 |
|
Hazard Ratio |
0.285 |
0.324 |
||
|
Log-rank Test p-value 3 |
<0.001 |
<0.001 |
||
|
Response |
||||
|
Complete Response (CR) n (%) |
23 (13) |
1 (1) |
27 (15) |
7 (4) |
|
Partial Response (RR/PR) n (%) |
84 (48) |
33 (19) |
77 (44) |
34 (19) |
|
Overall Response n (%) |
107 (61) |
34 (19) |
104 (59) |
41 (23) |
|
p-value |
<0.001 |
<0.001 |
||
|
Odds Ratio [95% CI] |
6.38 |
4.72 |
||
| a IPSS Risk Category: Low (combined score = 0), Intermediate-1 (combined score = 0.5 to 1), Intermediate-2 (combined score = 1.5 to 2.0), High (combined score ≥ 2.5); Combined score = (Marrow blast score + Karyotype score + Cytopenia score). b French-American-British (FAB) classification of MDS. |
||
|
Overall (N=148) |
||
|
Age (years) |
||
|
Median |
71 |
|
|
Min, Max |
37, 95 |
|
|
Gender |
n |
(%) |
|
Male |
51 |
(34.5) |
|
Female |
97 |
(65.5) |
|
Race |
n |
(%) |
|
White |
143 |
(96.6) |
|
Other |
5 |
( 3.4) |
|
Duration of MDS (years) |
||
|
Median |
2.5 |
|
|
Min, Max |
0.1, 20.7 |
|
|
Del 5 (q31-33) Cytogenetic Abnormality |
n |
(%) |
|
Yes |
148 |
(100) |
|
Other cytogenetic abnormalities |
37 |
(25.2) |
|
IPSS Score a |
n |
(%) |
|
Low (0) |
55 |
(37.2) |
|
Intermediate-1 (0.5-1.0) |
65 |
(43.9) |
|
Intermediate-2 (1.5-2.0) |
6 |
( 4.1) |
|
High (≥2.5) |
2 |
( 1.4) |
|
Missing |
20 |
(13.5) |
|
FAB Classification b from central review |
n |
(%) |
|
RA |
77 |
(52) |
|
RARS |
16 |
(10.8) |
|
RAEB |
30 |
(20.3) |
|
CMML |
3 |
( 2) |
| a ECOG = Eastern Cooperative Oncology Group. b MIPI = MCL International Prognostic Index. c High tumor burden is defined as at least one lesion that is ≥5 cm in diameter or 3 lesions that are ≥3 cm in diameter. d Bulky disease is defined as at least one lesion that is ≥7cm in the longest diameter. |
|
|
Baseline Disease Characteristics and Prior Anti -Lymphoma Treatment |
Total Patients (N=134) |
|
ECOG Performance Statusa n (%) |
|
|
0 |
43 (32) |
|
1 |
73 (54) |
|
2 |
17 (13) |
|
3 |
1 (<1) |
|
Advanced MCL Stage, n (%) |
|
|
III |
27 (20) |
|
IV |
97 (72) |
|
High or Intermediate MIPI Score b, n (%) |
90 (67) |
|
High Tumor Burdenc, n (%) |
77 (57) |
|
Bulky Diseased, n (%) |
44 (33) |
|
Extranodal Disease, n (%) |
101 (75) |
|
Number of Prior Systemic Anti-Lymphoma Therapies, n (%) |
|
|
Median (range) |
4 (2, 10) |
|
1 |
0 (0) |
|
2 |
29 (22) |
|
3 |
34 (25) |
|
≥ 4 |
71 (53) |
|
Number of Subjects Who Received Prior Regimen Containing, n (%): |
|
|
Anthracycline/mitoxantrone |
133 (99) |
|
Cyclophosphamide |
133 (99) |
|
Rituximab |
134 (100) |
|
Bortezomib |
134 (100) |
|
Refractory to Prior Bortezomib, n (%) |
81 (60) |
|
Refractory to Last Prior Therapy, n (%) |
74 (55) |
|
Prior Autologous Bone Marrow or Stem Cell Transplant, n (%) |
39 (29) |
|
Response Analyses (N = 133) |
N (%) |
95% CI |
|
|
Overall Response Rate (IWRC) (CR + CRu +PR) |
34 (26) |
(18.4, 33.9) |
|
|
Complete Response (CR + CRu) |
9 (7) |
(3.1, 12.5) |
|
|
CR |
1 (1) |
||
|
CRu |
8 (6) |
||
|
Partial Response (PR) |
25 (19) |
||
|
Duration of Response (months) |
Median |
95% CI |
|
|
Duration of Overall Response (CR + CRu + PR) |
(N = 34) |
16.6 |
(7.7, 26.7) |
| Data Cutoff: 22 June 2018 (AUGMENT) and 1 May 2017 (MAGNIFY). a Defined by GELF criteria. b Patient had either 0 (n=2) or 1 prior systemic therapy. ECOG = Eastern Cooperative Oncology Group; FLIPI = follicular lymphoma international prognostic index |
|||
|
Parameter |
AUGMENT Trial |
MAGNIFY Trial |
|
|
REVLIMID + Rituximab (N=178) |
Rituximab + Placebo (Control Arm) (N=180) |
REVLIMID + Rituximab (N=222) |
|
|
Age (years) |
|||
|
Median (Max, Min) |
64 (26, 86) |
62 (35, 88) |
65 (35, 91) |
|
Age distribution, n (%) |
|||
|
<65 years |
96 (54) |
107 (59) |
103 (46) |
|
≥65 years |
82 (46) |
73 (41) |
119 (54) |
|
Sex, n (%) |
|||
|
Male |
75 (42) |
97 (54) |
122 (55) |
|
Female |
103 (58) |
83 (46) |
100 (45) |
|
Race |
|||
|
White |
118 (66) |
115 (64) |
206 (93) |
|
Other races |
54 (30) |
64 (36) |
14 (6) |
|
Not collected or reported |
6 (3) |
1 (0.6) |
2 (1) |
|
Body Surface Area (BSA, m2) |
|||
|
Median (Max, Min) |
1.8 (1.4, 3.1) |
1.8 (1.3, 2.7) |
2 (1.3, 2.6) |
|
Disease Type FL or MZL |
|||
|
Follicular lymphoma |
147 (83) |
148 (82) |
177 (80) |
|
Marginal zone lymphoma |
31 (17) |
32 (18) |
45 (20) |
|
MZL subtype at diagnosis (investigator), n (%) |
|||
|
MALT |
14 (45) |
16 (50) |
10 (22) |
|
Nodal |
8 (26) |
10 (31) |
25 (56) |
|
Splenic |
9 (29) |
6 (19) |
10 (22) |
|
FL stage at diagnosis (investigator), n (%) |
|||
|
FL Grade 1-2 |
125 (85) |
123 (83) |
149 (84) |
|
FL Grade 3a |
22 (15) |
25 (17) |
28 (16) |
|
FLIPI score at baseline (calculated), n (%) |
Not Collected |
||
|
Low risk (0,1) |
52 (29) |
67 (37) |
|
|
Intermediate risk (2) |
55 (31) |
58 (32) |
|
|
High risk (≥3) |
69 (39) |
54 (30) |
|
|
Missing |
2 (1) |
1 (0.6) |
|
|
ECOG score at baseline, n (%) |
|||
|
0 |
116 (65) |
128 (71) |
102 (46) |
|
1 |
60 (34) |
50 (28) |
113 (51) |
|
2 |
2 (1) |
2 (1) |
7 (3) |
|
High tumor burdena at baseline, n (%) |
|||
|
Yes |
97 (54) |
86 (48) |
148 (67) |
|
No |
81 (46) |
94 (52) |
74 (33) |
|
Number of prior systemic antilymphoma therapies |
|||
|
1 |
102 (57) |
97 (54) |
94 (42)b |
|
>1 |
76 (43) |
83 (46) |
128 (58) |
| a Median estimate is from Kaplan-Meier analysis. b hazard ratio and its CI were estimated from Cox proportional hazard model adjusting for the stratification 3: previous rituximab treatment (yes, no), time since last antilymphoma therapy (≤ 2, > 2 years), and disease histology (FL, MZL). c p-value from log-rank test stratified by 3 factors noted above: previous rituximab treatment (yes, no), time since last antilymphoma therapy (≤ 2, > 2 years), and disease histology (FL, MZL). d Exact confidence interval for binomial distribution. |
||
|
Parameter |
REVLIMID + Rituximab (N=178) |
Rituximab + Placebo (N=180) |
|
PFS |
||
|
Patients with event, n (%) |
68 (38.2) |
115 (63.9) |
|
Death |
6 (8.8) |
2 (1.7) |
|
Progression of disease |
62 (91.2) |
113 (98.3) |
|
PFS, median a [95% CI] (months) |
39.4 [ 22.9, NE] |
14.1 [11.4, 16.7] |
|
HR b [95% CI] |
0.46 [ 0.34, 0.62] |
|
|
p-value c |
<0.0001 |
|
|
Objective response (CR+PR) , n(%) [95% CI] d |
138 (77.5) [70.7, 83.4] |
96 (53.3) [45.8, 60.8] |