What LEQVIO Contains
LEQVIO contains inclisiran sodium. This is a small interfering RNA (siRNA) medicine. It targets the PCSK9 protein in the body. Inclisiran has a special sugar (called GalNAc) attached that helps it reach liver cells. Most parts of inclisiran are modified with fluorine or methyl groups. Some parts have special linkages (phosphorothioate) for stability.
Molecular Details
The molecular formula is C529H664F12N176Na43O316P43S6. The molecular weight is 17,284.72 g/mol.
What It Looks Like
LEQVIO is a clear, colorless to pale yellow liquid. It is sterile and contains no preservatives. It comes in a prefilled syringe for injection under the skin. Each syringe contains 1.5 mL of solution with 284 mg of inclisiran (equivalent to 300 mg inclisiran sodium salt). The solution is made with Water for Injection and may contain small amounts of sodium hydroxide or phosphoric acid to adjust the pH to 7.0.
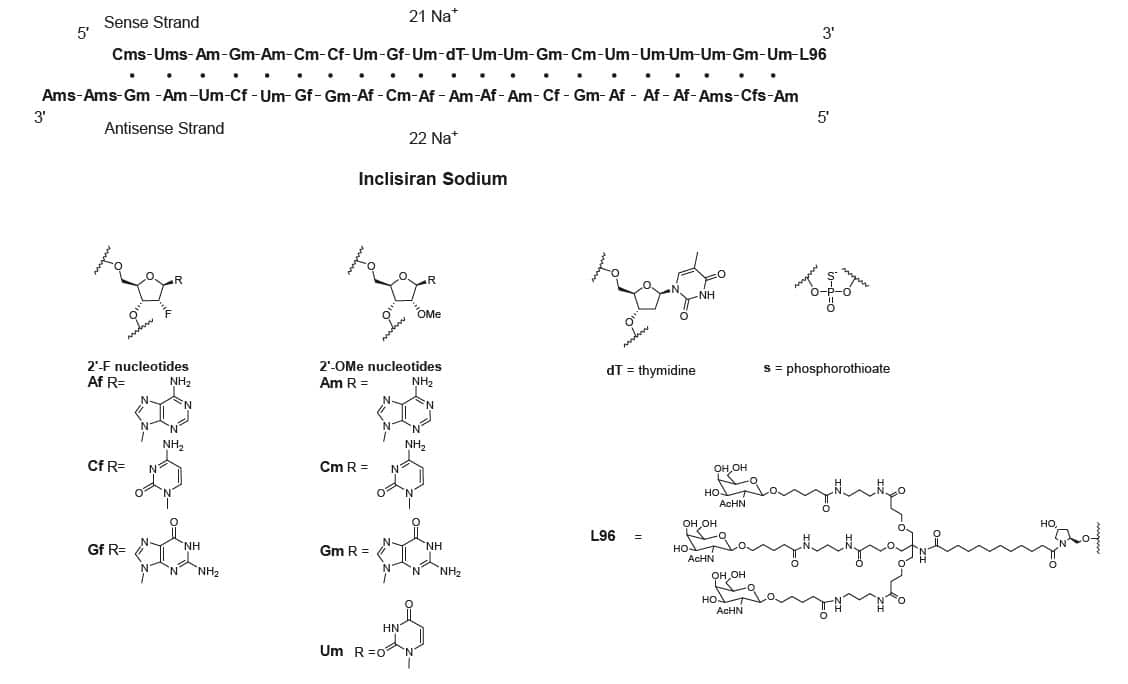
LEQVIO contains inclisiran sodium, a small interfering RNA (siRNA) directed to proprotein convertase subtilisin kexin type 9 (PCSK9) mRNA. Inclisiran contains a covalently linked ligand containing three N-acetylgalactosamine (GalNAc) residues to facilitate delivery to hepatocytes. With one exception, the 2’ribose moieties of the inclisiran sodium are present as 2′-F or 2′-OMe ribonucleotide. In addition, six of the terminal phosphodiester backbones are present as phosphorothioate linkages as indicated below.
The molecular formula of inclisiran sodium is C529H664F12N176Na43O316P43S6 and its molecular weight is 17,284.72 g/mol. It has the following structural formula:
Abbreviations: Af = adenine 2′-F ribonucleotide; Cf = cytosine 2′-F ribonucleotide; Gf = guanine 2′-F ribonucleotide; Am = adenine 2′-OMe ribonucleotide; Cm = cytosine 2′-OMe ribonucleotide; Gm = guanine 2′-OMe ribonucleotide; Um = uracil 2′-OMe ribonucleotide; L96 = triantennary GalNAc (N-acetyl-galactosamine)
LEQVIO is a sterile, preservative-free, clear, and colorless to pale yellow solution for subcutaneous use in a prefilled syringe. Each syringe contains 1.5 mL of solution containing the equivalent of 284 mg inclisiran (present as 300 mg inclisiran sodium salt). LEQVIO is formulated in Water for Injection and may also contain sodium hydroxide and/or phosphoric acid for pH adjustment to a target pH of 7.0.
Adults with Primary Hypercholesterolemia or HeFH
LEQVIO was studied in 3 main studies with 3,660 adults. All adults had high cholesterol and were already taking cholesterol medicine (statins) but needed more help lowering their LDL (bad) cholesterol. The studies compared LEQVIO to a placebo (inactive treatment).
Trial 1 – Adults with Heart Disease
Trial 1 (ORION-10) included 1,561 adults with heart disease. Patients received LEQVIO 284 mg or placebo as injections under the skin on Day 1, Day 90, Day 270, and Day 450. All patients were taking the highest dose of statin they could tolerate.
Patient details:
– Average age: 66 years
– 60% were 65 years or older
– 31% were female
– 45% had diabetes
– Average LDL-C at start: 105 mg/dL
– 89% were taking statin therapy
Results:
LEQVIO lowered LDL-C by 52% more than placebo at Day 510 (p < 0.0001).
Trial 2 – Adults with Heart Disease or High Risk
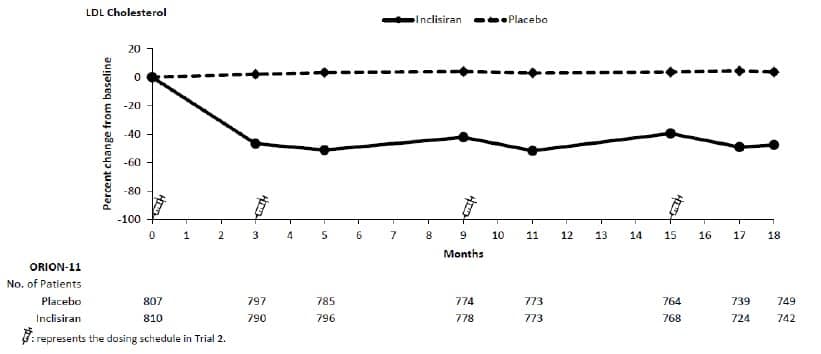
Trial 2 (ORION-11) included 1,617 adults with heart disease or high risk for heart disease. Patients received LEQVIO 284 mg or placebo as injections on Day 1, Day 90, Day 270, and Day 450.
Patient details:
– Average age: 65 years
– 55% were 65 years or older
– 28% were female
– 35% had diabetes
– Average LDL-C at start: 105 mg/dL
Results:
LEQVIO lowered LDL-C by 50% more than placebo at Day 510 (p < 0.0001).
Trial 3 – Adults with HeFH
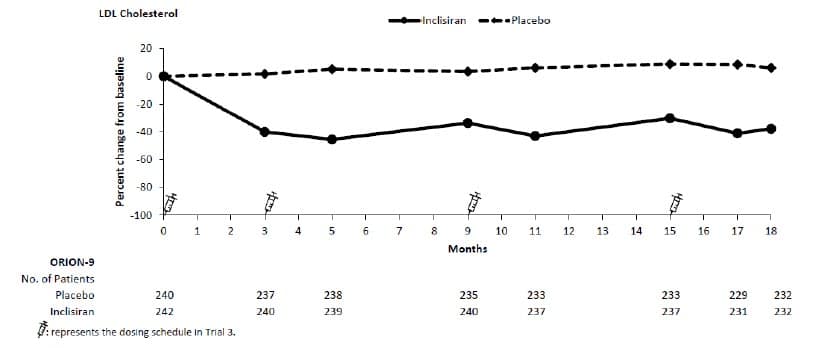
Trial 3 (ORION-9) included 482 adults with HeFH (a genetic form of high cholesterol). Patients received LEQVIO 284 mg or placebo as injections on Day 1, Day 90, Day 270, and Day 450.
Patient details:
– Average age: 55 years
– 22% were 65 years or older
– 53% were female
– 10% had diabetes
– Average LDL-C at start: 153 mg/dL
– 52% were also taking ezetimibe
Results:
LEQVIO lowered LDL-C by 48% more than placebo at Day 510 (p < 0.0001).
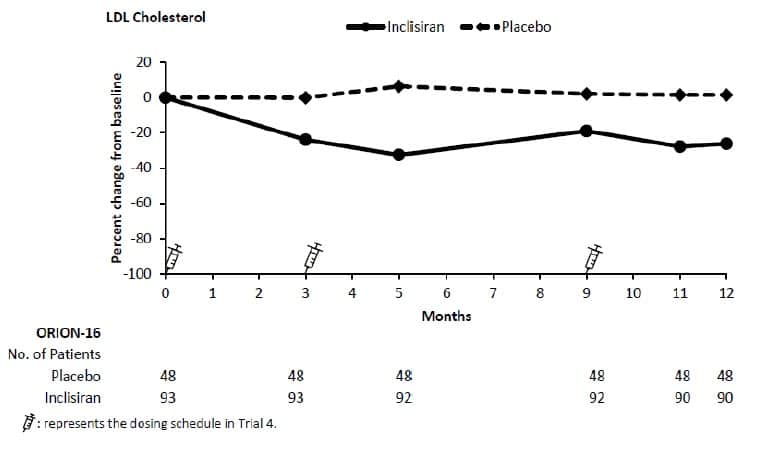
Trial 4 – Children with HeFH
Trial 4 (ORION-16) included 141 children ages 12 years and older with HeFH. Patients received LEQVIO 284 mg or placebo as injections on Day 1, Day 90, and Day 270.
Patient details:
– Average age: 15 years
– 53% were female
– Average LDL-C at start: 183 mg/dL
– 93% were taking statins
Results:
LEQVIO lowered LDL-C by 29% more than placebo at Day 330 (p < 0.0001).
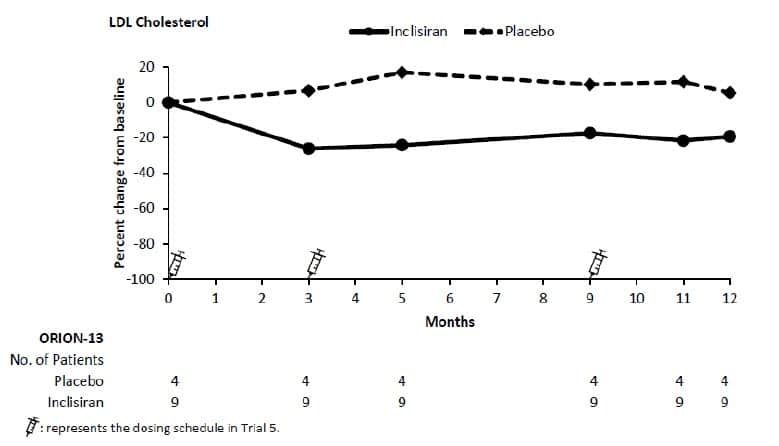
Trial 5 – Children with HoFH
Trial 5 (ORION-13) included 13 children ages 12 years and older with HoFH (a severe genetic form of high cholesterol). Patients received LEQVIO 284 mg or placebo as injections on Day 1, Day 90, and Day 270.
Patient details:
– Average age: 15 years
– 69% were female
– Average LDL-C at start: 272 mg/dL
Results:
LEQVIO lowered LDL-C by 33% more than placebo at Day 330. This study was very small and could not prove definite results.
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a11.5% of subjects on LEQVIO and 14.6% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using a mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 780) | 1 | 0 | 0 | -2 |
| LEQVIO (n = 781) | -51 | -34 | -47 | -45 |
| Difference from placebo (LS Mean) (95% CI) | -52 (-56, -49) |
-33 (-35, -31) |
-47 (-50, -44) |
-43 (-46, -41) |
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a10.6% of subjects on LEQVIO and 8.4% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 807) | 4 | 2 | 2 | 1 |
| LEQVIO (n = 810) | -46 | -28 | -41 | -38 |
| Difference from placebo (LS Mean) (95% CI) | -50 (-53, -47) |
-30 (-32, -28) |
-43 (-46, -41) |
-39 (-41, -37) |
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a4.5% of subjects on LEQVIO and 4.6% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value as a covariate. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 240) | 8 | 7 | 7 | 3 |
| LEQVIO (n = 242) | -40 | -25 | -35 | -33 |
| Difference from placebo (LS Mean) (95% CI) | -48 (-54, -42) |
-32 (-36, -28) |
-42 (-47, -37) |
-36 (-40, -32) |
| Treatment Group | LDL-C | ApoB | Non-HDL-C | Total Cholesterol |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a3.2% of subjects on LEQVIO and 0% of subjects on placebo had missing LDL-C data at primary endpoint (Day 330). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effects for treatment group and baseline age group, and baseline LDL-C as a covariate. Other endpoints were analyzed using same approach. |
||||
| Day 330 (mean percentage change from baseline)a | ||||
| Placebo (n = 48) | 1 | 4 | 2 | 0 |
| LEQVIO (n = 93) | -27 | -21 | -25 | -19 |
| Difference from placebo (LS Mean) (95% CI) | -29 (-36, -21) | -26 (-32, -20) | -27 (-34, -20) | -19 (-25, -14) |
| Treatment Group | LDL-C | ApoB | Non-HDL-C | Total Cholesterol |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
The trial was designed as a descriptive trial and was not powered to test any hypothesis. aNo subject in either LEQVIO or placebo had missing LDL-C data at primary endpoint (Day 330). No statistical model was performed. The mean and 95% CI of the difference from placebo were calculated based on a t-distribution for the percent change from baseline in LDL-C and other endpoints. |
||||
| Day 330 (mean percentage change from baseline)a | ||||
| Placebo (n = 4) | 12 | 5 | 9 | 9 |
| LEQVIO (n = 9) | -22 | -19 | -23 | -19 |
| Difference from placebo (Mean) (95% CI) | -33 (-80, 13) | -23 (-50, 4) | -33 (-87, 22) | -28 (-75, 19) |
Adults with Primary Hypercholesterolemia or HeFH
The efficacy of LEQVIO was investigated in three randomized, double-blind, placebo-controlled trials that enrolled 3,660 adults with HeFH, clinical ASCVD, or increased risk for ASCVD, who were taking maximally tolerated statin therapy and who required additional LDL-C lowering. Demographics and baseline disease characteristics were balanced between the treatment arms in all trials.
Adults with Primary Hypercholesterolemia
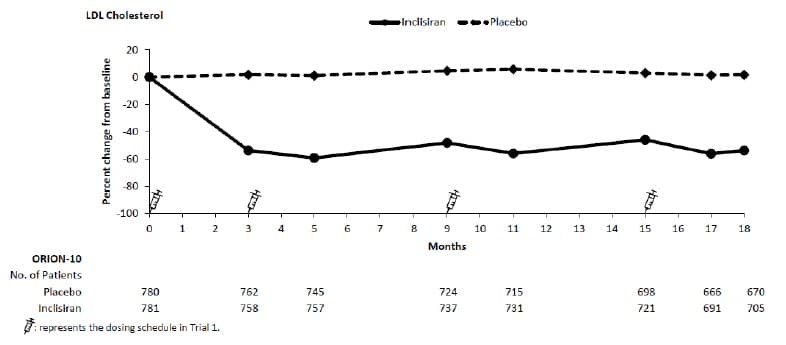
Trial 1 (ORION-10, NCT03399370) was a multicenter, double-blind, randomized, placebo-controlled 18-month trial in which 1,561 adults with ASCVD were randomized 1:1 to receive subcutaneous injections of either LEQVIO 284 mg (n = 781) or placebo (n = 780) on Day 1, Day 90, Day 270, and at Day 450. Patients were taking a maximally tolerated dose of statin with or without other lipid modifying therapy and required additional LDL-C reduction. Patients were stratified by current use of statins or other lipid-modifying therapies. Patients taking PCSK9 inhibitors were excluded from the trial.
The mean age at baseline was 66 years (range: 35 to 90 years), 60% were ≥65 years old, 31% were female, 86% were White, 13% were Black or African American, 1% were Asian, and 14% identified as Hispanic or Latino ethnicity. Forty-five percent (45%) of patients had diabetes at baseline. The mean baseline LDL-C was 105 mg/dL. At the time of randomization, 89% of patients were receiving statin therapy and 69% were receiving high-intensity statin therapy.
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a11.5% of subjects on LEQVIO and 14.6% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using a mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 780) | 1 | 0 | 0 | -2 |
| LEQVIO (n = 781) | -51 | -34 | -47 | -45 |
| Difference from placebo (LS Mean) (95% CI) | -52 (-56, -49) |
-33 (-35, -31) |
-47 (-50, -44) |
-43 (-46, -41) |
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a10.6% of subjects on LEQVIO and 8.4% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 807) | 4 | 2 | 2 | 1 |
| LEQVIO (n = 810) | -46 | -28 | -41 | -38 |
| Difference from placebo (LS Mean) (95% CI) | -50 (-53, -47) |
-30 (-32, -28) |
-43 (-46, -41) |
-39 (-41, -37) |
| Treatment Group | LDL-C | Total Cholesterol |
Non-HDL-C | ApoB |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a4.5% of subjects on LEQVIO and 4.6% of subjects on placebo had missing LDL-C data at primary endpoint (Day 510). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effect for treatment group and baseline LDL-C as a covariate. Other endpoints were analyzed using mixed-effect model for repeated measure (MMRM) with fixed effects for treatment group, visit, interaction between treatment and visit, and baseline value as a covariate. Missing data were imputed using a control-based pattern-mixture model approach. |
||||
| Day 510 (mean percentage change from baseline)a | ||||
| Placebo (n = 240) | 8 | 7 | 7 | 3 |
| LEQVIO (n = 242) | -40 | -25 | -35 | -33 |
| Difference from placebo (LS Mean) (95% CI) | -48 (-54, -42) |
-32 (-36, -28) |
-42 (-47, -37) |
-36 (-40, -32) |
| Treatment Group | LDL-C | ApoB | Non-HDL-C | Total Cholesterol |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
a3.2% of subjects on LEQVIO and 0% of subjects on placebo had missing LDL-C data at primary endpoint (Day 330). Missing data were imputed using a modified control-based multiple imputation to account for treatment adherence. Percent change from baseline in LDL-C was analyzed using analysis of covariance (ANCOVA) with fixed effects for treatment group and baseline age group, and baseline LDL-C as a covariate. Other endpoints were analyzed using same approach. |
||||
| Day 330 (mean percentage change from baseline)a | ||||
| Placebo (n = 48) | 1 | 4 | 2 | 0 |
| LEQVIO (n = 93) | -27 | -21 | -25 | -19 |
| Difference from placebo (LS Mean) (95% CI) | -29 (-36, -21) | -26 (-32, -20) | -27 (-34, -20) | -19 (-25, -14) |
| Treatment Group | LDL-C | ApoB | Non-HDL-C | Total Cholesterol |
|---|---|---|---|---|
| ApoB = apolipoprotein B; CI = confidence interval; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol
The trial was designed as a descriptive trial and was not powered to test any hypothesis. aNo subject in either LEQVIO or placebo had missing LDL-C data at primary endpoint (Day 330). No statistical model was performed. The mean and 95% CI of the difference from placebo were calculated based on a t-distribution for the percent change from baseline in LDL-C and other endpoints. |
||||
| Day 330 (mean percentage change from baseline)a | ||||
| Placebo (n = 4) | 12 | 5 | 9 | 9 |
| LEQVIO (n = 9) | -22 | -19 | -23 | -19 |
| Difference from placebo (Mean) (95% CI) | -33 (-80, 13) | -23 (-50, 4) | -33 (-87, 22) | -28 (-75, 19) |