Adult Rheumatoid Arthritis
Four main studies tested Enbrel in adults with rheumatoid arthritis (RA). RA is a disease that causes joint pain, swelling, and stiffness.
Study I
This study included 234 adults with active RA. Patients had tried at least one but no more than four other RA medicines without good results. They had at least 12 painful joints and 10 swollen joints. Patients received either 10 mg Enbrel, 25 mg Enbrel, or placebo (inactive pill) as a shot under the skin twice a week for 6 months.
Study II
This study included 89 adults with active RA who had also been taking a stable dose of methotrexate (MTX) for at least 6 months. They received either 25 mg Enbrel or placebo twice a week for 6 months, plus their regular MTX.
Study III
This study compared Enbrel to methotrexate in 632 adults with early active RA who had never taken methotrexate. Patients received either 10 mg Enbrel, 25 mg Enbrel, or methotrexate pills for 12 months. This study continued for up to 2 years.
Study IV
This study included 682 adults with RA lasting 6 months to 20 years. They had not responded well to at least one RA medicine (not including methotrexate). Patients were placed into three groups: methotrexate alone, Enbrel alone, or both Enbrel and methotrexate together.
Results in Rheumatoid Arthritis
More patients who took Enbrel showed improvement in their RA symptoms compared to those who took placebo or methotrexate alone. Improvement was measured using ACR scores (ACR 20, ACR 50, ACR 70). These scores show how much pain, swelling, and other symptoms improved:
– ACR 20 means at least 20% improvement
– ACR 50 means at least 50% improvement
– ACR 70 means at least 70% improvement
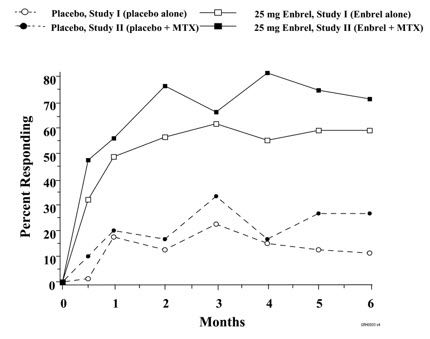
In Study I, at 6 months:
– 11% of placebo patients had ACR 20 improvement
– 59% of Enbrel patients had ACR 20 improvement
In Study III at 12 months:
– 65% of methotrexate patients had ACR 20 improvement
– 72% of Enbrel patients had ACR 20 improvement
In Study IV at 12 months:
– 59% of methotrexate alone patients had ACR 20 improvement
– 66% of Enbrel alone patients had ACR 20 improvement
– 75% of patients taking both Enbrel and methotrexate had ACR 20 improvement
The combination of Enbrel and methotrexate worked better than either medicine alone.
Most patients started to feel better within 1 to 2 weeks after starting Enbrel. Almost all patients who improved did so within 3 months.
After stopping Enbrel, RA symptoms usually came back within about 1 month. If patients started taking Enbrel again, they improved just as much as before.
Physical Function
The studies also measured how well patients could move and do daily activities. Patients taking Enbrel showed greater improvement in their ability to move and function compared to placebo. In Study I, patients went from having moderate trouble moving to having mild trouble moving after 6 months of Enbrel treatment.
X-Ray Results
Studies looked at joint damage using X-rays. In Study III, patients taking Enbrel had less joint damage progression compared to patients taking methotrexate. After 12 months, patients taking methotrexate had more joint damage (score of 1.59) compared to patients taking Enbrel (score of 1.00).
In Study IV, patients taking both Enbrel and methotrexate had the least joint damage progression.
Once Weekly Dosing
Another study tested giving 50 mg Enbrel as one shot once a week instead of two 25 mg shots twice a week. The results were similar to taking 25 mg twice a week.
—
Polyarticular Juvenile Idiopathic Arthritis
This study tested Enbrel in 69 children ages 2 to 17 with polyarticular JIA. This is a type of arthritis that affects many joints in children.
Children received Enbrel as a shot under the skin twice a week for 3 months. Then, children who responded well were split into two groups: one group kept taking Enbrel, and another group received placebo for 4 months.
Results showed:
– 51 of 69 children (74%) responded well to Enbrel and entered the next part of the study
– In the placebo group, 20 of 26 children (77%) had their disease flare up
– Only 6 of 25 children (24%) who kept taking Enbrel had a flare up
Children who kept taking Enbrel maintained their improvement. Many children who responded well to Enbrel continued to improve for up to 48 months.
—
Psoriatic Arthritis
This study tested Enbrel in 205 adults with psoriatic arthritis (PsA). PsA causes joint pain and swelling along with skin psoriasis.
Patients received either 25 mg Enbrel or placebo as a shot twice a week for 6 months.
Results at 6 months:
– 50% of Enbrel patients achieved ACR 20 improvement
– 13% of placebo patients achieved ACR 20 improvement
– 37% of Enbrel patients achieved ACR 50 improvement
– 4% of placebo patients achieved ACR 50 improvement
Improvements were seen as early as the first visit (4 weeks).
Skin psoriasis also improved. At 6 months:
– 47% of Enbrel patients had at least 50% improvement in their psoriasis skin score
– 18% of placebo patients had at least 50% improvement
Physical function also improved more in Enbrel patients. Patients taking Enbrel had a 54% improvement in their ability to do daily activities, compared to 6% in the placebo group.
X-rays showed that Enbrel slowed down joint damage. Most patients showed little or no change in joint damage over 24 months while taking Enbrel.
—
Ankylosing Spondylitis
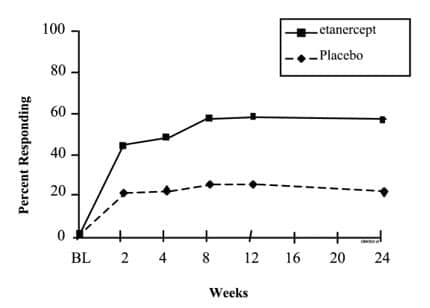
This study tested Enbrel in 277 adults with active ankylosing spondylitis. This is a type of arthritis that mainly affects the spine.
Patients received either 25 mg Enbrel or placebo as a shot twice a week for 6 months.
Results at 12 weeks:
– 60% of Enbrel patients achieved ASAS 20 improvement
– 27% of placebo patients achieved ASAS 20 improvement
– 45% of Enbrel patients achieved ASAS 50 improvement
– 13% of placebo patients achieved ASAS 50 improvement
Similar results were seen at 6 months. Enbrel helped reduce back pain, stiffness, and improved function.
—
Adult Plaque Psoriasis
Two studies tested Enbrel in adults with moderate to severe plaque psoriasis. This is a skin condition that causes red, scaly patches.
Study I
672 adults received either placebo or Enbrel at different doses for 3 months. After 3 months, placebo patients started taking Enbrel, and the study continued for another 3 months.
Results at 3 months:
– 4% of placebo patients had at least 75% improvement in their psoriasis (PASI 75)
– 14% of patients taking 25 mg once a week had PASI 75
– 32% of patients taking 25 mg twice a week had PASI 75
– 47% of patients taking 50 mg twice a week had PASI 75
Higher doses worked better.
Study II
611 adults received either placebo or Enbrel for 3 months.
Results at 3 months:
– 3% of placebo patients had PASI 75
– 32% of patients taking 25 mg twice a week had PASI 75
– 46% of patients taking 50 mg twice a week had PASI 75
Most patients who responded well to Enbrel kept their improvement when they continued treatment. Patients who stopped Enbrel usually had their psoriasis come back within 1 to 2 months.
—
Pediatric Plaque Psoriasis
This study tested Enbrel in 211 children ages 4 to 17 with moderate to severe plaque psoriasis.
Children received either Enbrel or placebo as a shot once a week for 12 weeks. After 12 weeks, all children received Enbrel for 24 more weeks.
Results at 12 weeks:
– 11% of placebo patients had at least 75% improvement in psoriasis
– 57% of Enbrel patients had at least 75% improvement
At 12 weeks:
– 13% of placebo patients had clear or almost clear skin
– 52% of Enbrel patients had clear or almost clear skin
Children who kept taking Enbrel maintained their improvement. When children who responded well were taken off Enbrel for 12 weeks, 65% still kept their improvement compared to 49% of those who switched to placebo.
| Placebo-Controlled | Active-Controlled | |||||
|---|---|---|---|---|---|---|
| Study I | Study II | Study III | ||||
| Placebo | Enbrel* | MTX/Placebo | MTX/Enbrel* | MTX | Enbrel* | |
| Response | N = 80 | N = 78 | N = 30 | N = 59 | N = 217 | N = 207 |
| ACR 20 | ||||||
| Month 3 | 23% | 62%† | 33% | 66%† | 56% | 62% |
| Month 6 | 11% | 59%† | 27% | 71%† | 58% | 65% |
| Month 12 | NA | NA | NA | NA | 65% | 72% |
| ACR 50 | ||||||
| Month 3 | 8% | 41%† | 0% | 42%† | 24% | 29% |
| Month 6 | 5% | 40%† | 3% | 39%† | 32% | 40% |
| Month 12 | NA | NA | NA | NA | 43% | 49% |
| ACR 70 | ||||||
| Month 3 | 4% | 15%† | 0% | 15%† | 7% | 13%‡ |
| Month 6 | 1% | 15%† | 0% | 15%† | 14% | 21%‡ |
| Month 12 | NA | NA | NA | NA | 22% | 25% |
| Endpoint | MTX (N = 228) |
Enbrel (N = 223) |
Enbrel/MTX (N = 231) |
|---|---|---|---|
|
|||
| ACR N*, † | |||
| Month 12 | 40% | 47% | 63%‡ |
| ACR 20 | |||
| Month 12 | 59% | 66% | 75%‡ |
| ACR 50 | |||
| Month 12 | 36% | 43% | 63%‡ |
| ACR 70 | |||
| Month 12 | 17% | 22% | 40%‡ |
| Major Clinical Response§ | 6% | 10% | 24%‡ |
|
|

| Placebo N = 80 |
Enbrel*
N = 78 |
|||
|---|---|---|---|---|
| Parameter (median) | Baseline | 3 Months | Baseline | 3 Months† |
|
||||
| Number of tender joints ‡ | 34.0 | 29.5 | 31.2 | 10.0§ |
| Number of swollen joints ¶ | 24.0 | 22.0 | 23.5 | 12.6§ |
| Physician global assessment # | 7.0 | 6.5 | 7.0 | 3.0§ |
| Patient global assessment # | 7.0 | 7.0 | 7.0 | 3.0§ |
| Pain # | 6.9 | 6.6 | 6.9 | 2.4§ |
| Disability index Þ | 1.7 | 1.8 | 1.6 | 1.0§ |
| ESR (mm/hr) | 31.0 | 32.0 | 28.0 | 15.5§ |
| CRP (mg/dL) | 2.8 | 3.9 | 3.5 | 0.9§ |
| MTX | 25 mg Enbrel | MTX/Enbrel (95% Confidence Interval*) |
P Value | ||
|---|---|---|---|---|---|
|
|||||
| 12 Months | Total Sharp Score | 1.59 | 1.00 | 0.59 (-0.12, 1.30) | 0.1 |
| Erosion Score | 1.03 | 0.47 | 0.56 (0.11, 1.00) | 0.002 | |
| JSN Score | 0.56 | 0.52 | 0.04 (-0.39, 0.46) | 0.5 | |
| 6 Months | Total Sharp Score | 1.06 | 0.57 | 0.49 (0.06, 0.91) | 0.001 |
| Erosion Score | 0.68 | 0.30 | 0.38 (0.09, 0.66) | 0.001 | |
| JSN Score | 0.38 | 0.27 | 0.11 (-0.14, 0.35) | 0.6 | |
| MTX (N = 212)* |
Enbrel (N = 212)* |
Enbrel/MTX (N = 218)* |
|
|---|---|---|---|
| Total Sharp Score (TSS) | 2.80 (1.08, 4.51) |
0.52†
(-0.10, 1.15) |
-0.54‡,§
(-1.00, -0.07) |
| Erosion Score (ES) | 1.68 (0.61, 2.74) |
0.21†
(-0.20, 0.61) |
-0.30‡
(-0.65, 0.04) |
| Joint Space Narrowing (JSN) Score | 1.12 (0.34, 1.90) |
0.32 (0.00, 0.63) |
-0.23‡,§
(-0.45, -0.02) |
| Placebo N = 104 |
Enbrel*
N = 101 |
|||
|---|---|---|---|---|
| Parameter (median) | Baseline | 6 Months | Baseline | 6 Months |
|
||||
| Number of tender joints† | 17.0 | 13.0 | 18.0 | 5.0 |
| Number of swollen joints‡ | 12.5 | 9.5 | 13.0 | 5.0 |
| Physician global assessment§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Patient global assessment§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Morning stiffness (minutes) | 60 | 60 | 60 | 15 |
| Pain§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Disability index¶ | 1.0 | 0.9 | 1.1 | 0.3 |
| CRP (mg/dL)# | 1.1 | 1.1 | 1.6 | 0.2 |
| Figure 2. ASAS 20 Responses in Ankylosing Spondylitis |
|---|
 |
| Placebo N = 139 |
Enbrel*
N = 138 |
|||
|---|---|---|---|---|
| Median values at time points | Baseline | 6 Months | Baseline | 6 Months |
|
||||
| ASAS response criteria | ||||
| Patient global assessment † | 63 | 56 | 63 | 36 |
| Back pain ‡ | 62 | 56 | 60 | 34 |
| BASFI § | 56 | 55 | 52 | 36 |
| Inflammation ¶ | 64 | 57 | 61 | 33 |
| Acute phase reactants | ||||
| CRP (mg/dL) # | 2.0 | 1.9 | 1.9 | 0.6 |
| Spinal mobility (cm): | ||||
| Modified Schober’s test | 3.0 | 2.9 | 3.1 | 3.3 |
| Chest expansion | 3.2 | 3.0 | 3.3 | 3.9 |
| Occiput-to-wall measurement | 5.3 | 6.0 | 5.6 | 4.5 |
| Placebo/Enbrel | Enbrel/Enbrel | |||
|---|---|---|---|---|
| 25 mg BIW | 25 mg QW | 25 mg BIW | 50 mg BIW | |
| (N = 168) | (N = 169) | (N = 167) | (N = 168) | |
| 3 Months | ||||
| PASI 75 n (%) | 6 (4%) | 23 (14%)* | 53 (32%)† | 79 (47%)† |
| Difference (95% CI) |
10% (4, 16) | 28% (21, 36) | 43% (35, 52) | |
| sPGA, “clear” or “minimal” n (%) | 8 (5%) | 36 (21%)† | 53 (32%)† | 79 (47%)† |
| Difference (95% CI) |
17% (10, 24) | 27% (19, 35) | 42% (34, 50) | |
| PASI 50 n (%) | 24 (14%) | 62 (37%)† | 90 (54%)† | 119 (71%)† |
| Difference (95% CI) |
22% (13, 31) | 40% (30, 49) | 57% (48, 65) | |
| 6 Months | ||||
| PASI 75 n (%) | 55 (33%) | 36 (21%) | 68 (41%) | 90 (54%) |
| Placebo | Enbrel | ||
|---|---|---|---|
| 25 mg BIW | 50 mg BIW | ||
| (N = 204) | (N = 204) | (N = 203) | |
|
|||
| PASI 75 n (%) | 6 (3%) | 66 (32%)* | 94 (46%)* |
| Difference (95% CI) | 29% (23, 36) | 43% (36, 51) | |
| sPGA, “clear” or “minimal” n (%) | 7 (3%) | 75 (37%)* | 109 (54%)* |
| Difference (95% CI) | 34% (26, 41) | 50% (43, 58) | |
| PASI 50 n (%) | 18 (9%) | 124 (61%)* | 147 (72%)* |
| Difference (95% CI) | 52% (44, 60) | 64% (56, 71) | |
| Placebo (N = 105) |
Enbrel 0.8 mg/kg Once Weekly (N = 106) |
|
|---|---|---|
| PASI 75, n (%) | 12 (11%) | 60 (57%) |
| PASI 90, n (%) | 7 (7%) | 29 (27%) |
| sPGA “clear” or “almost clear” n (%) | 14 (13%) | 55 (52%) |
14.1 Adult Rheumatoid Arthritis
The safety and efficacy of Enbrel were assessed in four randomized, double-blind, controlled studies. The results of all four trials were expressed in percentage of patients with improvement in RA using ACR response criteria.
Study I evaluated 234 patients with active RA who were ≥ 18 years old, had failed therapy with at least one but no more than four disease-modifying antirheumatic drugs (DMARDs) (e.g. hydroxychloroquine, oral or injectable gold, MTX, azathioprine, D-penicillamine, sulfasalazine), and had ≥ 12 tender joints, ≥ 10 swollen joints, and either erythrocyte sedimentation rate (ESR) ≥ 28 mm/hr, C-reactive protein (CRP) > 2.0 mg/dL, or morning stiffness for ≥ 45 minutes. Doses of 10 mg or 25 mg Enbrel or placebo were administered SC twice a week for 6 consecutive months.
Study II evaluated 89 patients and had similar inclusion criteria to Study I except that patients in Study II had additionally received MTX for at least 6 months with a stable dose (12.5 to 25 mg/week) for at least 4 weeks and they had at least 6 tender or painful joints. Patients in Study II received a dose of 25 mg Enbrel or placebo SC twice a week for 6 months in addition to their stable MTX dose.
Study III compared the efficacy of Enbrel to MTX in patients with active RA. This study evaluated 632 patients who were ≥ 18 years old with early (≤ 3 years disease duration) active RA, had never received treatment with MTX, and had ≥ 12 tender joints, ≥ 10 swollen joints, and either ESR ≥ 28 mm/hr, CRP > 2.0 mg/dL, or morning stiffness for ≥ 45 minutes. Doses of 10 mg or 25 mg Enbrel were administered SC twice a week for 12 consecutive months. The study was unblinded after all patients had completed at least 12 months (and a median of 17.3 months) of therapy. The majority of patients remained in the study on the treatment to which they were randomized through 2 years, after which they entered an extension study and received open-label 25 mg Enbrel. MTX tablets (escalated from 7.5 mg/week to a maximum of 20 mg/week over the first 8 weeks of the trial) or placebo tablets were given once a week on the same day as the injection of placebo or Enbrel doses, respectively.
Study IV evaluated 682 adult patients with active RA of 6 months to 20 years duration (mean of 7 years) who had an inadequate response to at least one DMARD other than MTX. Forty-three percent of patients had previously received MTX for a mean of 2 years prior to the trial at a mean dose of 12.9 mg. Patients were excluded from this study if MTX had been discontinued for lack of efficacy or for safety considerations. The patient baseline characteristics were similar to those of patients in Study I. Patients were randomized to MTX alone (7.5 to 20 mg weekly, dose escalated as described for Study III; median dose 20 mg), Enbrel alone (25 mg twice weekly), or the combination of Enbrel and MTX initiated concurrently (at the same doses as above). The study evaluated ACR response, Sharp radiographic score, and safety.
Clinical Response
| Placebo-Controlled | Active-Controlled | |||||
|---|---|---|---|---|---|---|
| Study I | Study II | Study III | ||||
| Placebo | Enbrel* | MTX/Placebo | MTX/Enbrel* | MTX | Enbrel* | |
| Response | N = 80 | N = 78 | N = 30 | N = 59 | N = 217 | N = 207 |
| ACR 20 | ||||||
| Month 3 | 23% | 62%† | 33% | 66%† | 56% | 62% |
| Month 6 | 11% | 59%† | 27% | 71%† | 58% | 65% |
| Month 12 | NA | NA | NA | NA | 65% | 72% |
| ACR 50 | ||||||
| Month 3 | 8% | 41%† | 0% | 42%† | 24% | 29% |
| Month 6 | 5% | 40%† | 3% | 39%† | 32% | 40% |
| Month 12 | NA | NA | NA | NA | 43% | 49% |
| ACR 70 | ||||||
| Month 3 | 4% | 15%† | 0% | 15%† | 7% | 13%‡ |
| Month 6 | 1% | 15%† | 0% | 15%† | 14% | 21%‡ |
| Month 12 | NA | NA | NA | NA | 22% | 25% |
| Endpoint | MTX (N = 228) |
Enbrel (N = 223) |
Enbrel/MTX (N = 231) |
|---|---|---|---|
|
|||
| ACR N*, † | |||
| Month 12 | 40% | 47% | 63%‡ |
| ACR 20 | |||
| Month 12 | 59% | 66% | 75%‡ |
| ACR 50 | |||
| Month 12 | 36% | 43% | 63%‡ |
| ACR 70 | |||
| Month 12 | 17% | 22% | 40%‡ |
| Major Clinical Response§ | 6% | 10% | 24%‡ |
|
|
| Placebo N = 80 |
Enbrel*
N = 78 |
|||
|---|---|---|---|---|
| Parameter (median) | Baseline | 3 Months | Baseline | 3 Months† |
|
||||
| Number of tender joints ‡ | 34.0 | 29.5 | 31.2 | 10.0§ |
| Number of swollen joints ¶ | 24.0 | 22.0 | 23.5 | 12.6§ |
| Physician global assessment # | 7.0 | 6.5 | 7.0 | 3.0§ |
| Patient global assessment # | 7.0 | 7.0 | 7.0 | 3.0§ |
| Pain # | 6.9 | 6.6 | 6.9 | 2.4§ |
| Disability index Þ | 1.7 | 1.8 | 1.6 | 1.0§ |
| ESR (mm/hr) | 31.0 | 32.0 | 28.0 | 15.5§ |
| CRP (mg/dL) | 2.8 | 3.9 | 3.5 | 0.9§ |
| MTX | 25 mg Enbrel | MTX/Enbrel (95% Confidence Interval*) |
P Value | ||
|---|---|---|---|---|---|
|
|||||
| 12 Months | Total Sharp Score | 1.59 | 1.00 | 0.59 (-0.12, 1.30) | 0.1 |
| Erosion Score | 1.03 | 0.47 | 0.56 (0.11, 1.00) | 0.002 | |
| JSN Score | 0.56 | 0.52 | 0.04 (-0.39, 0.46) | 0.5 | |
| 6 Months | Total Sharp Score | 1.06 | 0.57 | 0.49 (0.06, 0.91) | 0.001 |
| Erosion Score | 0.68 | 0.30 | 0.38 (0.09, 0.66) | 0.001 | |
| JSN Score | 0.38 | 0.27 | 0.11 (-0.14, 0.35) | 0.6 | |
| MTX (N = 212)* |
Enbrel (N = 212)* |
Enbrel/MTX (N = 218)* |
|
|---|---|---|---|
| Total Sharp Score (TSS) | 2.80 (1.08, 4.51) |
0.52†
(-0.10, 1.15) |
-0.54‡,§
(-1.00, -0.07) |
| Erosion Score (ES) | 1.68 (0.61, 2.74) |
0.21†
(-0.20, 0.61) |
-0.30‡
(-0.65, 0.04) |
| Joint Space Narrowing (JSN) Score | 1.12 (0.34, 1.90) |
0.32 (0.00, 0.63) |
-0.23‡,§
(-0.45, -0.02) |
| Placebo N = 104 |
Enbrel*
N = 101 |
|||
|---|---|---|---|---|
| Parameter (median) | Baseline | 6 Months | Baseline | 6 Months |
|
||||
| Number of tender joints† | 17.0 | 13.0 | 18.0 | 5.0 |
| Number of swollen joints‡ | 12.5 | 9.5 | 13.0 | 5.0 |
| Physician global assessment§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Patient global assessment§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Morning stiffness (minutes) | 60 | 60 | 60 | 15 |
| Pain§ | 3.0 | 3.0 | 3.0 | 1.0 |
| Disability index¶ | 1.0 | 0.9 | 1.1 | 0.3 |
| CRP (mg/dL)# | 1.1 | 1.1 | 1.6 | 0.2 |
| Figure 2. ASAS 20 Responses in Ankylosing Spondylitis |
|---|
|
| Placebo N = 139 |
Enbrel*
N = 138 |
|||
|---|---|---|---|---|
| Median values at time points | Baseline | 6 Months | Baseline | 6 Months |
|
||||
| ASAS response criteria | ||||
| Patient global assessment † | 63 | 56 | 63 | 36 |
| Back pain ‡ | 62 | 56 | 60 | 34 |
| BASFI § | 56 | 55 | 52 | 36 |
| Inflammation ¶ | 64 | 57 | 61 | 33 |
| Acute phase reactants | ||||
| CRP (mg/dL) # | 2.0 | 1.9 | 1.9 | 0.6 |
| Spinal mobility (cm): | ||||
| Modified Schober’s test | 3.0 | 2.9 | 3.1 | 3.3 |
| Chest expansion | 3.2 | 3.0 | 3.3 | 3.9 |
| Occiput-to-wall measurement | 5.3 | 6.0 | 5.6 | 4.5 |
| Placebo/Enbrel | Enbrel/Enbrel | |||
|---|---|---|---|---|
| 25 mg BIW | 25 mg QW | 25 mg BIW | 50 mg BIW | |
| (N = 168) | (N = 169) | (N = 167) | (N = 168) | |
| 3 Months | ||||
| PASI 75 n (%) | 6 (4%) | 23 (14%)* | 53 (32%)† | 79 (47%)† |
| Difference (95% CI) |
10% (4, 16) | 28% (21, 36) | 43% (35, 52) | |
| sPGA, “clear” or “minimal” n (%) | 8 (5%) | 36 (21%)† | 53 (32%)† | 79 (47%)† |
| Difference (95% CI) |
17% (10, 24) | 27% (19, 35) | 42% (34, 50) | |
| PASI 50 n (%) | 24 (14%) | 62 (37%)† | 90 (54%)† | 119 (71%)† |
| Difference (95% CI) |
22% (13, 31) | 40% (30, 49) | 57% (48, 65) | |
| 6 Months | ||||
| PASI 75 n (%) | 55 (33%) | 36 (21%) | 68 (41%) | 90 (54%) |
| Placebo | Enbrel | ||
|---|---|---|---|
| 25 mg BIW | 50 mg BIW | ||
| (N = 204) | (N = 204) | (N = 203) | |
|
|||
| PASI 75 n (%) | 6 (3%) | 66 (32%)* | 94 (46%)* |
| Difference (95% CI) | 29% (23, 36) | 43% (36, 51) | |
| sPGA, “clear” or “minimal” n (%) | 7 (3%) | 75 (37%)* | 109 (54%)* |
| Difference (95% CI) | 34% (26, 41) | 50% (43, 58) | |
| PASI 50 n (%) | 18 (9%) | 124 (61%)* | 147 (72%)* |
| Difference (95% CI) | 52% (44, 60) | 64% (56, 71) | |
| Placebo (N = 105) |
Enbrel 0.8 mg/kg Once Weekly (N = 106) |
|
|---|---|---|
| PASI 75, n (%) | 12 (11%) | 60 (57%) |
| PASI 90, n (%) | 7 (7%) | 29 (27%) |
| sPGA “clear” or “almost clear” n (%) | 14 (13%) | 55 (52%) |